
Help! My voice is _____!
There are several causes of voice disorders. Causes may be organic (structural or neurologic), functional, psychogenic, or a combination of them. Possible causes are listed on this website to help educate, not diagnose! Possible treatment options are there to give information about what speech therapy might look like. This website can help you be informed as you meet with Speech-Language Pathologists, Otolaryngologists, Neurologists, or other medical professionals.
Help! My Voice is BREATHY!
Possible causes
What is it?
The SLP might refer to it as “breathy phonation.” It is incomplete adduction of the vocal folds. In other words, your vocal folds are not closing all the way or closing enough. The vocal folds are not vibrating efficiently, so they are wasting air, making you sound breathy.

(Vocal Cords, n.d.)
The SLP will likely refer you to an ENT to help determine the cause and make sure your vocal folds are healthy. Below are a few possible causes of breathy phonation.
-
Vocal Nodules
-
Most common benign type of lesion.
-
They are usually very responsive to speech therapy!
-
Surgery is the last option.
-
See the image on the right to see how they prevent the vocal folds from adducting completely.
-
-
Vocal Fold Polyps
-
Fluid-filled lesions.
-
Often require surgery, but you may be able to try speech therapy first.
-
See the image on the right to see how they prevent the vocal folds from adducting completely.
-
-
Neurological Disorders
-
Examples: Recurrent Laryngeal Nerve Paralysis, Parkinson’s Disease, Myasthenia Gravis.
-
-
Inappropriate or excessive vocal use.
-
Consistently engaging in poor vocal hygiene.
-

(Vocal Fold Lesions, ,2017)
How it might be treated
Treatment depends on the cause and is designed individually on a case by case basis. Your ENT will help determine the course of action if there is a pathology at the level of the vocal folds, such as nodules or polyps. If nodules are present, you will likely try speech therapy. If polyps are present, the ENT may have you try speech therapy, but often they require surgery. If you have nodules or polyps and participate in speech therapy, the SLP will first educate you about your vocal folds and how to take care of them using good vocal hygiene. The SLP may also have you try speaking with glottal fry. Glottal fry is not the speech goal, however, it will help you relax the vocal folds (Voice Disorders, n.d.). For many people, they have breathy phonation due to inappropriate or excessive vocal use. People who are required to use their vocal folds often and loudly, such as teachers or singers, may find that they have breathy phonation. If it is inappropriate vocal use, the SLP will teach you how to firmly engage your vocal folds so they adduct properly. Have you ever tried to push something very heavy? Try it now. Do you feel your vocal folds close? That’s approximation. You and the SLP will work to learn how to appropriately approximate, not too hard and not too soft. You will likely also work on increasing your intensity. When you are loud, you force your vocal folds to approximate! The SLP will also help train your ears to know the difference between when vocal folds are approximating correctly and when they are not. You may also learn how to do a hard glottal attack. This is where the vocal folds are squeezed too hard. So you would then modify that to create an appropriate approximation. The SLP may also have you engage in negative practice. This is where you would purposely be breathy, and then purposefully use your good, nonbreathy voice! The SLP will also help you understand how to have good vocal hygiene. Click here to learn more about vocal hygiene!
What is it?
If people are having difficulty hearing you, even in a quiet environment, you may have reduced loudness. We make our voices loud by having adequate subglottal air pressure and by approximating our vocal folds. Speaking too softly can be because of an imbalance between the airflow and the muscle activity (Stemple, 2014). Speaking too softly can even cause vocal trauma if the airstream is not supporting the vocal folds well enough (Stemple, 2014).
Possible causes
The SLP will likely first refer you to an Audiologist for a complete hearing evaluation. The SLP may also refer to an ENT to help determine the cause and make sure your vocal folds are healthy. Below are a few possible causes of decreased intensity.
-
Hearing Loss
-
Conductive hearing loss may cause you to speak too quietly.
-
-
Muscle Tension Dysphonia
-
Visible tension in the throat, neck, shoulders, and jaw.
-
Causes pain in larynx and neck.
-
-
Ventricular Phonation
-
The ventricular folds are drawn to midline.
-
Usually happens when true vocal folds do not function properly.
-
-
Neurological Disorders
-
Examples: Parkinson’s Disease, Myasthenia Gravis, or injury to the superior laryngeal nerve or the recurrent laryngeal nerve (see image to the right to see how the nerves innervate the larynx).
-
-
Vocal Fatigue
-
Usually no neurological or structural problem.
-
Deteriorated voice quality and endurance.
-
Effortful voice production.
-
Help! My Voice is QUIET!
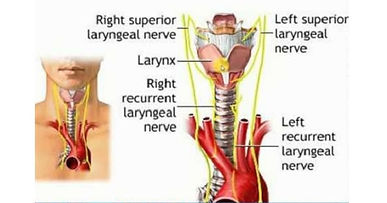
(Laryngeal Nerve Supply, n.d.)
How it might be treated
Treatment depends on the cause and is designed individually on a case by case basis. If it is not an auditory issue, the SLP will likely first increase your awareness of the problem. The SLP may record your voice so you can compare your intensity to an average intensity. The SLP may also discuss with you what the adverse effects are on your vocal folds as well as on your relationships. For example, speaking too quietly may cause people to ignore you or end a conversation early. Then you may practice direct manipulation using short phrases. The SLP may record these to use for you to train your ears (Stemple, 2014). Then you will be able to auditorily discriminate between adequate intensity and too low intensity. The SLP may also integrate the use of a hand-held sound level meter. This will display your intensity so that you can train productions at a reasonable level and stabilize them. You may start with words and work your way to phrases, paragraphs, and conversational speech (Stemple, 2014). Auditory masking is another approach that the SLP might use. Have you noticed when you're in a noisy environment, people tend to automatically talk louder? This is called the Lombard effect. In order to help you speak louder, the SLP may have you wear headphones that produce masking noise while you talk or read passages (Voice Disorders, n.d.).
Since treatment is dependent on the cause, treatment will look different if the cause is Parkinson's Disease. For example, the SLP may use The Lee Silverman Voice Treatment (LSVT) program. The LSVT is the most studied of all voice therapy programs (Stemple, 2014) and is often used for people with Parkinson's Disease. It is an intensive treatment program focusing on improving intensity. Click here to learn more about the program.
Help! My Voice is NASALLY!
What is it?
If it sounds like your voice is coming out of your nose too much (think Steve Urkel), you may have hypernasality. Hyponasality is when it sounds like not enough voice is going through your nose (think about having a bad cold and being very "stuffed up"). In English, the sounds "m" as in "mom," "n" as in "no", and "ng" as in "ring" all are nasal sounds. The sound should come through the nasal cavity. All other sounds should go through the oral cavity. When many sounds are going through the nasal cavity that should not be, you will sound hypernasal. In the phrase "please pet the puppy," there are no nasal sounds. By putting a mirror under your nose and saying the phrase, you can see if any air is coming through the nasal cavity because it will create fog on the mirror. Tonsillectomy and adenoidectomies may have effects on resonance.
Possible causes
The SLP will likely refer you to an ENT to help determine the cause and make sure your vocal folds velopharyngeal valve are healthy. Below are a few possible causes of nasal speech.
-
Velopharyngeal Dysfunction (VPD)
-
Cleft palate
-
even after it is repaired.
-
-
Irregular adenoids
-
Surgery may be recommended.
-
-
Neurogenic causes
-
Traumatic brain injury, stroke, cerebral palsy.
-
-
Velopharyngeal Mislearning
-
learned misarticulations (Resonance Disorders, n.d.).
-
-
Functional resonance problem
-
inconsistent resonance, but stimulable for normal resonance.
-

(Cleft lip and palate, 2009)
How it might be treated
Treatment depends on the cause and is designed individually on a case by case basis. If it is a functional resonance problem, the SLP will likely spend time educating you about hypernasality. Then you may learn how to auditorily differentiate between normal resonance and hypernasality. Although articulation is not the issue at hand, working on articulation may help generate better resonance. Maximizing the strength and coordination of your articulators will help force the air out through the oral cavity because your mouth will be opening wider. You may also work on pitch and loudness. Decreasing your pitch and increasing your intensity can also help force the air out through the oral cavity. You may even get to work on some nonspeech sounds, such as animal or engine noises! The SLP will help you shape these nonnasal sounds into words to practice saying words without hypernasality. The SLP may assess your articulation to find if there are other sounds produced without nasal resonance. These sounds can be incorporated into words and phrases to help facilitate normal resonance. To generate a feeling for speaking without hypernasality, you can try speaking like you have a cold. By acting "stuffed up," you will likely occlude the nasal cavity and all the sounds will go through the oral cavity, which is in opposition to hypernasality. You may also purposefully speak with hypernasality and then speak with normal resonance, using the negative practice to solid normal resonance. There are also instruments that can give feedback as to resonance to you know when you are getting it correct, such as a nasometer- seen below.

(Mayo,2011)
Good Vocal Hygiene
What is it?
This is how you take care of your vocal folds. It is eliminating or modifying traumatic vocal behaviors and instilling healthy vocal behaviors. It is often combined with other treatments to ensure vocal health. Work with your SLP to determine which poor behaviors you engage in and why, what impact those behaviors have, and how they can be eliminated or modified.
Traumatic Behaviors
These behaviors are considered poor vocal hygiene
-
Shouting
-
Talking loudly
-
Throat clearing
-
Coughing
-
Smoking
-
Drug/alcohol use
-
Caffeinated beverages
-
Poor hydration
-
Breathing in chemicals, dust, or other irritants (Stemple, 2014)
-
Grunting during exercise (Stemple, 2014)
-
Prolonged talking
Healthy Behaviors
Replace or modify traumatic behaviors with these.
-
Drink plenty of water
-
avoid caffeinated beverages
-
-
Do not smoke and avoid smokey environments
-
Rest the voice regularly
-
Take vocal naps (Stemple, 2014)
-
-
Instead of clearing your throat, try swallowing or drinking water
-
Instead of talking loudly to be above the noise, reduce background noise, move to a different environment, or move closer to the listener
-
Use amplification when speaking in a large room or to many people (Stemple, 2014)
-
Cough quietly
-
Do not sing lower or higher than what is comfortable
-
do not sing if there is pain when singing or swallowing (Stemple, 2014)
-
Vocal naps are short periods of no talking throughout the day (Stemple, 2014). These are important after a big performance or a day with many vocal demands. The naps should be spread out over the following two or three days. This allows for tissue regeneration (Stemple, 2014).
Vocal Naps
References
American Speech-Language-Hearing Association. (n.d.). Resonance Disorders (Practice Portal). Retrieved April 24, 2020, from https://www.asha.org/PRPSpecificTopic.aspx?folderid=8589943934§ion
American Speech-Language-Hearing Association. (n.d.). Voice Disorders (Practice Portal). Retrieved April 24, 2020, from https://www.asha.org/PRPSpecificTopic.aspx?folderid=8589942600§ion=Treatment
Cleft lip and palate. (2009). Retrieved from https://www.aboutkidshealth.ca/Article?contentid=380&language=English#
Laryngeal Nerve Supply. (n.d.). Retrieved from https://medicoapps.org/m-laryngeal-nerve-supply/
Mayo, C. M., & Mayo, R. (2011). Nasometer. Retrieved from https://libres.uncg.edu/ir/uncg/f/R_Mayo_Normative_2011.pdf
Stemple, J. C., Roy, N., & Klaben, B. (2014). Clinical voice pathology: theory and management. San Diego, CA: Plural Publishing.
Vocal Cords. (n.d.). Retrieved from https://study.com/academy/lesson/phonation-definition-process.html
Vocal Fold Lesions. (2017). Retrieved from https://www.bouldervoicelessons.com/blog/scarynodes